Let me be honest with you.
No nursing school prepared me for the moment a patient looked me directly in the eye and requested a very specific cocktail of controlled drugs, then screamed the entire ward down when I paused to check whether giving them simultaneously was safe.
There I stood, barely weeks post-orientation, heart doing its best impression of a SpO2 alarm on a restless patient, thinking: they absolutely did not cover this in the OSCE.
And here is what I have since learned: that experience is not mine alone. It is happening in NHS wards every shift. It is happening in Australian public hospitals where methamphetamine presentations in acute care have risen sharply. It is happening in New Zealand DHBs and Health New Zealand localities where opioid dispensing rates have doubled over the past decade.
This is not a niche ward problem. It is a mainstream nursing issue, and it deserves a proper clinical conversation.
Why This Conversation Matters
Substance use disorder (SUD) does not discriminate by admission reason or postcode.
It walks through every hospital door.
A patient admitted for a fractured NOF at 02:00. The chest infection in bay three. The post-op review who flags a complex drug history on admission and watches you clock it.
In the UK, hospital admissions linked to drug-related conditions have risen year on year. Nurses in acute settings encounter patients with active SUD regularly, yet formal training on managing these interactions remains thin.
In Australia, the pressure is measurable. 84% of methamphetamine-related ED presentations are managed entirely within the ED, with a median stay of 14 hours, meaning the nurse on that shift is carrying the full clinical and behavioural load of that presentation from arrival to discharge. In New Zealand, the pattern holds.
As nurses, we are the last clinical line before a medication reaches a patient's vein. Yet the conversation in clinical spaces is still dominated by discomfort and judgment rather than strategy, compassion, and actual skill.
A Quick Clarification Before We Go Further
This guide is not about the chronic pain patient with a documented opioid tolerance, the palliative patient who needs adequate symptom control, or the post-surgical patient whose pain is being inadequately managed. Those are important but different conversations.
This guide is specifically about the clinical and ethical complexity that arises when a patient with active or suspected SUD is admitted for an unrelated condition and you are the nurse responsible for their analgesia. That requires a different toolkit.
Six Strategies That Will Actually Help You at the Bedside
1. Check Your Bias, or It Will Check You
Before you pull up the drug chart, ask yourself an honest question: am I walking into this room with a verdict already written?
Patients with SUD have often accumulated significant trauma, systemic neglect, and chronic stigma, including from healthcare workers. When they sense judgment, communication breaks down fast and your shift gets harder.
Rember, as a nurse, empathy is not the same as enabling.
You can hold both: I understand you are in pain, and I am going to administer this safely. Patients who sense judgment from their nurse disengage, withhold information, and are more likely to self-discharge before treatment is complete. The bias is not just unkind. It is clinically unsafe.
2. Know Your Scope Because You Cannot Fix This in One Shift
This mindset shift protects more nurses from burnout than almost anything else.
You are not their GP, their counsellor, or their addiction specialist. Your role is to provide safe, evidence-based nursing care, manage pain within what is prescribed, document clearly, communicate concerns through proper channels, and treat the person in front of you with basic human dignity.
That is where you stand. That is also enough.
3. Avoid the Power Struggle Because There Is No Version You Win
If you withhold prescribed medication to assert control, you are causing unnecessary suffering and likely breaching your NMC, AHPRA, or Nursing Council obligations. If you administer beyond what is safe to end the conflict, you are putting both the patient and your PIN at serious risk.
Stay clinical. Use calm, authoritative language.
"I can see you are in a lot of pain. I am going to give you what has been prescribed, and if that is not managing it adequately, I will escalate to the medical team to review the plan."
That sentence validates the patient's experience, is clinically honest, and closes the negotiation without a confrontation.
4. Escalate Early and Document Everything
If the pain management plan is not working, that is a clinical escalation, not a personal negotiation.
Document precisely:
-
Exact words used when requesting medication
-
Pain scores both self-reported and observed
-
Your assessment of sedation level
-
Respiratory rate and conscious state
-
Every conversation with the medical team
-
What was actioned.
In the NHS, use SBAR every time. In Australia, escalation pathways like REACH and COMPASS exist for exactly this. In New Zealand, know your locality's escalation protocol and use it. If a registrar dismisses a documented concern, document that too.
Your documentation is your professional protection. Sparse notes after a complex SUD interaction are a liability.
5. Use the Interdisciplinary Team Because That Is What They Are There For
In the NHS, many trusts now have specialist substance misuse liaison nurses in acute settings. Request them early, not as a last resort. In Australia, most tertiary hospitals have Alcohol and Other Drugs (AOD) services for bedside consults. In New Zealand, DHBs and Health New Zealand localities have addiction medicine services for complex presentations.
Pharmacists are particularly underused in these conversations. They can review the full chart, flag interactions, and advise on appropriate alternatives. A patient with complex SUD should have a clear MDT plan within 24 hours. If it does not exist, escalate until it does.

6. Give a Clinical, Judgment-Free Handover
How you hand over a patient shapes how the next nurse will treat them for the rest of their admission.
Judgemental: "Bed 6 is a drug seeker, watch yourself."
Clinical: "Bed 6 has a documented history of opioid use disorder. Pain management has been complex this shift. I have escalated to the registrar, documented fully, and she responds well to calm communication with clear timeframes around medication."
The first primes the next nurse for a power struggle before they have met the patient. The second gives clinical information that actually helps. The language we use in handover shapes ward culture over time.
Situation and Action: The Quick Reference
|
Situation |
What Not to Do |
What to Do Instead |
|
Patient demands specific drug and route |
Refuse out of frustration |
Administer what is prescribed; escalate if inadequate |
|
Patient becomes aggressive |
Argue or capitulate |
Use calm, factual language; call for support |
|
Pain score does not match presentation |
Dismiss as drug-seeking |
Document both; escalate to the medical team |
|
Handover is complex and draining |
Use stigmatising shorthand |
Use clinical, objective language |
|
You feel manipulated or unsafe |
Internalise it |
Debrief with a senior; document; escalate |
The Bottom Line
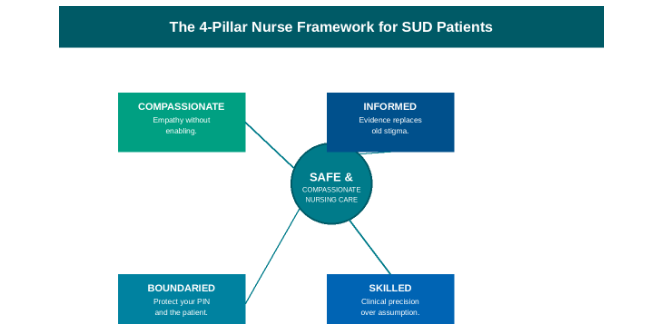
Caring for patients with SUD is one of the most clinically and emotionally complex experiences you will have as a nurse. It asks you to be compassionate, because the patient is a human being in pain.
Boundaried, because your registration and their safety depend on it. Skilled, because this is a clinical challenge, not a personal one. And informed, because the old narratives around drug-seeking are both harmful and outdated.
The nurses who navigate this well are not the ones who got lucky with an easy patient. They are the ones who walked in prepared.
That is exactly what UKNurses is here to help you do, whether you are working nights in an NHS trust, managing a busy shift in an Australian ED, or building your nursing career across the Tasman in New Zealand.
Ready to take the next step in your nursing career? Book an appointment with UKNurses and get personalised support today.